
NURBN2026 Nursing Practice Report
Please use information below to structure your case report:
Gloria’s situation (100 words):
Briefly identify what you know about Gloria. Describe or list facts and context and relevant features of Glorias situation. Consider Gloria’s situation focusing on her current health, recent past health history and social circumstances.
Collect cues (300 words)
After reading through Gloria Johnson’s case study, what relevant cues and information can you identify? For example, what current information is of interest (review), what significant signs and symptoms do you notice about Gloria’s clinical presentation (review), recall related knowledge of Glorias health issues including pathophysiology, pharmacology and epidemiology (recall).
Gather what other information or assessments might provide useful information for Gloria’s care. For example, observations, interviews, exams or diagnostic tools (gather)? Include a brief rationale for each cue or information you identify as being of relevance.
Reflect (150 words):
Critically review your own practice and identify areas for refinement, improvement and/or change
What did you learn by completing this case report?
Where do you need to focus your efforts for wider understanding?
George Thompson, a 68-year-old male patient, is to be admitted for dehydration noted after his third chemotherapy cycle for stage III pancreatic cancer for which he received chemotherapy 8 days ago. He suffers from severe fatigue, nausea, and lack of appetite resulting in weight loss and minimal oral intake therefore dehydrated. During the assessment the patient is pale and weak, his lips are cracked and mucous membranes are dry, and he says urine output has been scanty lately. Overall HR assessment: Mild dehydration – skin turgor, capillary refill time, and oral mucosa are appropriate; Lab: Neutropenia – Neutrophils: 0.6 x 10^9/L. George has a stable home married life, and good social support but has limited desire to eat and suffers several unfavorable effects of chemotherapy that would slow down his recovery process (Kidney Health Australia, 2024).

(Source: Case scenario)
Current Information and Observations
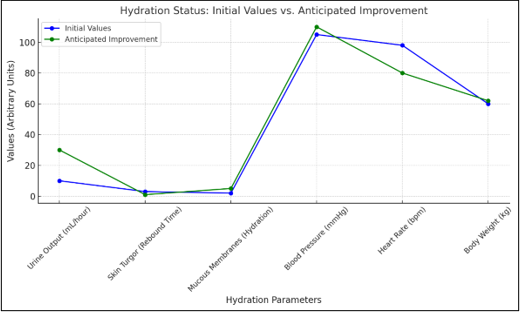
1. Physical Symptoms: Common symptoms suggestive of dehydration include tiredness, dry and sticky saliva, sore and chapped lips, and little or less frequent urination. These can be indicative of low levels of hydration that, coupled with such nausea liable to reduce oral intake further, are likely to be more severe.
2. Vital Signs: A normal blood pressure of 105/80 mmHg and respiratory rate of 98 bpm show mild compensation made by the body to dehydration. Although not severe, they should be carefully watched in order not to exacerbate (Australian Government Department of Health, 2022).
3. Lab Results: An absolute neutrophil count of 0.6 x 10^9/L defines severe neutropenia essentially raising George’s vulnerability to infections. This warrants, immediate neutropenic precautions and frequent surveillance for symptoms of infections.
1. Pancreatic Cancer and Chemotherapy: George's chemotherapy drugs such as fluorouracil are cytotoxic and can affect all sorts of dividing cells hence causing side effects such as nausea, fatigue, neutropenia, and weight loss.
2. Dehydration: Presumably due to poor oral intake, chronic nausea, and other side effects of chemotherapy such as vomiting or diarrhea. This dehydration worsens his tiredness as well as general emaciation.
3. Malnutrition: During chemotherapy, both George’s fatigue as well as loss of weight demonstrate malnutrition as a complication. Lack of basic nutrients resulting from poor diet affects his recovery as well as the overall performance of his immune system.
1. Fluid Status: In particular, the intake and output are measured and compared periodically to determine the patient's level of hydration. Failure to do this will allow conclusion-making on whether one is retaining or losing fluids much as weighing the body on a daily basis will assist in identifying changes. More information can be gathered from turgor skin and capillary refill time to support the assessment for hydration (Cancer Council Australia, 2021).
2. Nutritional Screening: Individuals can complete a screening tool like the MST, or the SGA to quantify the calorie/protein deficiencies in George's experience. Determine his willingness or need for oral nutrition, or if a change under the label of diet change is needed.
3. Infection Screening: Hyponeutropenia in turn directs the need to check temperature frequently, preferably every 4-6 hours. Other clues, like inflammation or redness within the specific infected area, and severe pain, might be present even if classic symptoms in this case are absent.
Another strength, as part of his care plan, is that George is married and his wife is supportive. However, they were stigmatized physically, emotionally, and psychologically by both George and his wife when facing cancer treatment. These include such chronic effects as fatigue, nausea, and changes in appetite that may give patients a feeling of frustration or even helplessness (Berardi et al., 2019).
Rationale
Among them three sets of cues for MBA assignment expert are identified; the first is hydration status, the second is the risk of infection and the third one is nutritional deficiencies These are important because they help in the formulation of George's care plan. The shelter is sought first to relieve a person's symptoms and arrest progression of the compromising at the physiological level. The patient is neutropenic and, therefore, at a very high risk of problems developing from any infection. Malnutrition needs to be addressed to enhance energy and immunologic function, as well as to facilitate healing, which needs supplementation. The social and emotional aspects are just important as well since the treatment of the psychological aspects may also improve George's compliance and other Clients' recovery process.
.png)
.png)
.png)
(Source: Author)
Identify Abnormalities
1. Dehydration: Inability to exclude alcohol ingestion, hypotension, dry skin, furred tongue, and desquamated lips and cracked oral mucosa, decreased output, diminished skin turgor are evidence of dehydration. Such symptoms coupled with his continued complaints of nausea reveal that the main problem is likely to be inadequate oral fluid intake.
2. Neutropenia: An ANC of 0.6 x 10^9/L puts George at a higher risk of developing an infection. For example, due to CHOP chemotherapy-induced neutropenia, he is at a high risk of developing infections including those that are resistant to common protection measures in a hospital (Mandal et al., 2022).
3. Nausea and Weight Loss: By experiencing and sustaining nausea, weight, and appetite loss and reduction, an individual suffers from nutritional loss. Fatigue can be dramatically worsened by malnutrition, and the length of time required for recovery may be significantly prolonged.
Relevant Information:
Physical signs: Factors that are obvious indicators of dehydration include cracked lips, dryness of the mucous membrane, and fatigue.
Laboratory results: Neutrophil count identifies a sharp surgical infection risk.
Symptoms: Nausea and decreased oral intake significantly underscore why nutritional and antinausea therapies should not leave the clinician’s treatment arsenal (Ravasco, 2019).
Irrelevant Information:
Stable oxygen saturation: A reading of 98% on room air means no respiratory distress.
Normal hemoglobin and platelet levels: These parameters are however insignificant in the current state of George’s picture with reference to his general health.
Hydration Issues: The signs include dryness of the mucous membrane, scanty urine, rough and cracked lips, and when the skin, when pinched, barely springs back are some of the common signs illustrative of dehydration. This is probably worsened by nausea that has for instance restricted George's fluid intake (Virizuela et al., 2017).
Infection Risk: Absolute neutrophil count below this range is particularly critical to indicate that the patient is at a high risk of acute infection. This is because his immune system is compromised by both the hospital environment and his chemotherapy treatment.
Nutritional Deficits: Nausea at a persistent level together with loss of weight accompanied by little or no oral intake means the patient requires nutritional management. These cues revolve around the side effects of chemotherapy and show the importance of time-sensitive strategies.
1. Dehydration: Due to lack of fluids, vomiting, and possible effects of chemotherapy on one's intestinal tract. If left untreated then the condition in patients can aggravate and create issues like electrolyte alterations and poor perfusion of organs.
2. Risk of Infection: Chemotherapy-induced neutropenia directly related to it. Hospital exposure raises infection risks, hence strict infection control measures are needed.
3. Nutritional Deficits: Probably due to chemo-induced vomiting and lethargy, coupled with poor appetite and weight loss (Kalkan et al., 2018).
1. Electrolyte Levels: Knowledge of the patient’s electrolyte status would give clues about any problems arising from the dehydrated state.
2. Infection Signs: Composite evaluation, particularly regarding signs of mild infection (e.g., erythema in specific areas, tachycardia), is required owing to neutropenia.
3. Nutritional Details: A quantitative determination of the degree of malnutrition was lacking; a qualitative description of food intake, or dietary analysis, would probably have been more useful.
1. Dehydration Management: Clinical practice guidelines call for standard IV rehydration for moderate to severe cases of dehydration if the patient cannot take fluids orally for some time. Ondansetron may help decrease nausea and thus enhance oral Lyte and nutrient consumption (NICE, 2022).
2. Neutropenic Precautions: Infection control measures for neutropenic patients include place isolation measures, proper hand washing, and keeping away from crowded places or people with infections. Research reveals that neutropenic patients are advantaged to be given antibiotics once infections start rer, (Smith et al., 2020).
3. Nutritional Interventions: Cancer patients with malnutrition have been reported to do poorer than well-nourished patients; their capacity to withstand treatment is lower, and their quality of life is less than that of better-nourished patients. As with other strategies of nausea and fatigue, nutritional supplementation is also critical. Enteral feeding or high-calorie, high-protein diets should be used in severe cases as recommended by the Cancer Council Australia (2021).
1. To treat the problem of hydration, the patient needs to receive intravenous fluids to replenish the body’s fluids. The last requirement necessary for measuring and controlling organizational effectiveness involves the continuous observation of inputs and outcomes.
2. The interventions surrounding infection risks include neutropenic measures, observation for the early signs of infections, and teaching George/ the family measures to take at home to prevent infections (Van Soom et al., 2020)
3. Nutrition interventions require the formulation of nutritional support measures that help eradicate feeding deficiencies. These may include, eating several, but small meals daily, administration of antiemetics to help address the problem of nausea, and inviting a dietician to recommend special diet intake.
The three major nursing diagnosing focuses for George are: Hydration, Infection, and the risk of Malnutrition. All of these symptoms are related directly to his chemotherapy treatment and these symptoms focus that a multimodal, individualized evidence-based care plan should be used for this patient. About these areas comprehensiveness, nursing care enhances the recovery process, reduces the chances of complications, and reduces the amount of discomfort that George will experience during chemotherapy.
Acute Nursing Problem
This degenerates after adequate oral intake is not provided, and due to persistent nausea, most probably from chemotherapy. Moderate dehydration is characterized by physical symptoms of cracked lips, dry and pale mucous membranes, reduced urine output, and fatigue. If left untreated, then dehydration results in an alteration of the electrolyte balance, decreased peripheral organ blood flow, and other secondary events. For George, he needs to be given intravenous fluids, and antiemetics to reduce cases of nausea and vomiting as well as constant check up on his fluid levels in a bid to reverse this condition (Armer, 2020).
Potential Nursing Problem
George has severe neutropenia, which is expressed by a neutrophil count of 0.6 x 10^9/L, which is therefore considered at high risk for infection due to this side effect of chemotherapy. Neutropenia affects his immunity therefore making him a candidate for opportunistic infections especially in hospital. Since the infection can be asymptomatic even at this stage, the need for strict infection control measures cannot be exaggerated including neutropenic precautions, daily screenings for fever or localized skin erythema, and constant patient education on hygiene. This is why George's doctor should be sensitive to managing those early stages and avoid any further health problems that could complicate his health during chemotherapy. This risk should be constantly controlled and probably will require special attention and coordination with the healthcare team.
Establish goals
1. Acute Problem Goal: Increase the intake of fluids within the next 24 hours by giving George / IV fluids, observing the fluid balance, oral intake, and examples could include increased urine output/ improved mucous membranes.
2. Potential Problem Goal: Decrease the infection rate within the next 48 hours by instituting neutropenic precautions, teaching George and his wife about any precautions against infections, and checking for signs of infection.
Acute Problem: Dehydration
1. IV Fluids Administration
To treat moderate dehydration common with George's condition, intravenous fluids must be given. This intervention will contribute to adding flow back to the intravascular total body volume, correct the imbalance of the electrolyte, and enhance the perfusion of organs. The type and rate of IV fluids should match the ordered schedule, of course, paying attention to possible signs of fluid overload, for example, edema or changes in respiratory status. The guidelines which are from NICE (2022) also support the use of isotonic fluids in the management of patients with chemotherapy-induced dehydration.
2. Anti-Emetic Therapy
These comprise ondansetron or any other anti-emetic that will be very useful in control of the chemotherapy-induced nausea in George's case. It will also help him improve the way he tolerates oral intake as this will not cause him much discomfort. Ondansetron is known to prevent serotonin receptors in the gastrointestinal system which are often triggered by chemotherapy. These are supplemented with the authors noting that antiemetics enhances and manages nausea and adequate fluid intake.
3. Oral Rehydration
Shaping George to drink ORS solutions often works familiarization with IV treatment and improves the gradual shift in the levels of fluid regeneration. ORS hold electrolytes hence useful in replacement of the losses at the same time being non-irritating to the G.I. tract. It is advisable to give small quantities of fluids regularly to build tolerance to fluids as the side effects of nausea reduce.
Potential Problem: Infection Risk
1. Neutropenic Precautions
Because of George’s severely low neutrophil count, or neutropenia, neutropenic precautions are necessary to avoid an infection. These are; washing hands with instructions to CARs to wash their hands thoroughly before and after handling the children, minimizing the number of visitors to the facility to reduce the spreading of infectious diseases, and using aseptic procedures in any invasive procedures on the children. Giving him a private room if possible also reduces his contact with other patient's sources of infection thus reducing Hospital-acquired infections.
2. Education
George and his wife need to be taught more about how infections work and a way through which they can be detected early. They should understand the symptoms of infection for the area which include fever, redness, or pain at the site of injection, and should be advised to seek further medical attention if any of the symptoms are realized. More instructions will be given and stressing the students to comprehend what has been written will enrich this learning.
3. Regular Monitoring
Temperature check every four hours and monitoring for other minor infection indications mean that any infection is detected immediately to be dealt with appropriately. He further said that with frequent follow up the level of infection does not advance to the next stage which is very important for immunocompromised patients (Kidney Health Australia, 2024).
1. Dietary Support
Also because of the loss of weight by the patient and a decrease in appetite, a referral to a dietitian is required. George can opt for a high protein high calorie diet formulated by the dietitian to bring him the nutrition he lost while aiding in recovery.
2. Oral Nutrition Supplements
Oral nutritional support products like protein or calorie-dense liquids can easily fill in the gap between George’s ideal caloric intake and the amount of calories he is consuming. Supplements should be appetizing and introduced slowly for the sake of not overloading his appetite due to reduced appetite.
Expected Outcomes
Hydration: By now I expect George to show an increase in urine output, skin turgor elasticity, and moist mucous membranes within 24 hours of intravenous fluids and oral rehydration therapy.
Infection: For the next 48+ hours he should be afebrile which means no signs of infection like swollen skin, redness, or a high white blood cell count.
Nutrition: Transient enamel demineralization and further enhancement of oral intake and weight that was maintained in the subsequent days by modifications to diet and nutrients.
All the interventions are based on the evidence-practice model to meet George's needs and possible hazards. Such goals address his dehydration issue while avoiding aggravations of it straight on. Measures with the patient that follow neutropenic precautions and educate the patient are consistent with immunocompromised patients. A little more about the care planning is that the nutritional care plans are individualized for George due to malnutrition, and weight loss to help combat the side effects of chemotherapy. These programs make sure that effective short-term goals are being achieved in relation to the long-term health care of participants (Cancer Council Australia, 2021).
Review
This case demonstrated the need for early assessment and intervention in relation to the risk of dehydration, infection, and risk of malnutrition in patients with cancer undergoing chemotherapy. George's case served to remind one how intervention contents controlled by nurses could dramatically alter the fortunes of even such a case.
Learning
Managing George's compound problems offered an understanding of the close relationship between the patient's hydration, immunity, and nutrition throughout oncology treatment. This made me realize how chemotherapy impacts the patients in their entirety and why the designs of a care plan need to consider different aspects of the patient. It also stressed not only the complications but also more patient and caregiver education in managing the disease.
Focus for Improvement
In the future, I would like to enhance my knowledge of oncology key concepts as well as enhance my skills in the approaches to the management of the severe manifestations and sequels in cancer patients. The identification of new information in nutrition support in oncology clients as well as the acquisition of improved competencies in coordination of care will enhance results in other clients like George.
Armer, J. (2020). ONS Guidelines™ for cancer treatment–related lymphedema. Oncology Nursing Forum, 47(5), 518-538. https://doi.org/10.1188/20.ONF.518-538
Australian Government Department of Health. (2022). Dehydration and its impact on health. Australian Government Department of Health. Retrieved from https://www.health.gov.au
Berardi, R., Torniai, M., Lenci, E., Pecci, F., Morgese, F., & Rinaldi, S. (2019). Electrolyte disorders in cancer patients: A systematic review. J Cancer Metastasis Treat, 5(79), 1-33. https://doi.org/10.4103/jcmt.jcmt_48_18
Cancer Council Australia. (2021). Chemotherapy and hydration. Cancer Council Australia. Retrieved from https://www.cancer.org.au
Kalkan, N. O., Almalı, A. O., Gokmen, A., & Dogan, E. (2018). Chemotherapy-induced tumour lysis syndrome in gastric adenocarcinoma with diffuse liver metastases: A case report. Journal of Cancer Therapy, 9(1), 16-22. https://doi.org/10.4236/jct.2018.91002
Kidney Health Australia. (2024). Dehydration and kidney health. Kidney Health Australia. Retrieved from https://kidney.org.au
Mandal, S., Naik, J., Vidya, J., Singh, P., Ram, A., & Arakeri, G. (2022). Self-reported minor chemotherapy adverse effects in cancer patients: Incidence and management. GRRBE, 8(1), 9-16. https://doi.org/10.1186/s43064-022-00099-w
NICE. (2022). Dehydration: Diagnosis and management in adults in primary and secondary care; National Institute for Health and Care Excellence. Retrieved from https://www.nice.org.uk/guidance/ng201
Ravasco, P. (2019). Nutrition in cancer patients. Journal of Clinical Medicine, 8(8), 1211. https://doi.org/10.3390/jcm8081211
Van Soom, T., El Bakkali, S., Gebruers, N., Verbelen, H., Tjalma, W., & van Breda, E. (2020). The effects of chemotherapy on energy metabolic aspects in cancer patients: A systematic review. Clinical Nutrition, 39(6), 1863-1877. https://doi.org/10.1016/j.clnu.2019.06.022
Virizuela, J. A., Camblor-Alvarez, M., Luengo-Pérez, L. M., Grande, E., Alvarez-Hernández, J., Sendrós-Madrono, M. J., ... & Ocón-Bretón, M. J. (2017). Nutritional support and parenteral nutrition in cancer patients: An expert consensus report. Retrieved from https://seom.org/seomcms/images/stories/recursos/Art_nutricion_en_cancer_Seccion_CC_oct2017.pdf



Essay: 10 Pages, Deadline: 2 days
They delivered my assignment early. They also respond promptly. This is excellent. Tutors answer my questions professionally and courteously. Good job. Thanks!
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Report: 10 Pages, Deadline: 4 days
After sleeping for only a few hours a day for the entire week, I was very weary and lacked the motivation to write anything or think about any suggestions for the writer to include in the paper. I am glad I chose your service and was pleasantly pleased by the quality. The paper is complete and ready for submission to the professor. Thanks!
![]() User ID: 9***85 United
States
User ID: 9***85 United
States
Assignment: 8 Pages, Deadline: 3 days
I resorted to the MBA assignment Expert in the hopes that they would provide different outcomes after receiving unsatisfactory results from other assignment writing organizations, and they genuinely are fantastic! I received exactly what I was looking for from this writing service. I'm grateful.
![]() User ID: 9***55
User ID: 9***55
Assignment: 13 Pages, Deadline: 3 days
Incredible response! I could not believe I had received the completed assignment so far ahead of the deadline. Their expert team of writers effortlessly provided me with high-quality content. I only received an A because of their assistance. Thank you very much!
![]() User ID: 6***15 United
States
User ID: 6***15 United
States
Essay: 8 Pages, Deadline: 3 days
This expert work was very nice and clean.expert did the included more words which was very kind of them.Thank you for the service.
![]() User
ID: 9***95 United
States
User
ID: 9***95 United
States
Report: 15 Pages, Deadline: 5 days
Cheers on the excellent work, which involved asking questions to clarify anything they were unclear about and ensuring that any necessary adjustments were made promptly.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Essay: 9 Pages, Deadline: 5 days
To be really honest, I can't bear writing essays or coursework. I'm fortunate to work with a writer who has always produced flawless work. What a wonderful and accessible service. Satisfied!
![]() User ID: 9***95
User ID: 9***95

Essay: 12 Pages, Deadline: 4 days
My essay submission to the university has never been so simple. As soon as I discovered this assignment helpline, however, everything improved. They offer assistance with all forms of academic assignments. The finest aspect is that there is also an option for escalation. We will get a solution on time.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
Essay: 15 Pages, Deadline: 3 days
This is my first experience with expert MBA assignment expert. They provide me with excellent service and complete my project within 48 hours before the deadline; I will attempt them again in the future.
![]() User ID: 9***95 United
States
User ID: 9***95 United
States
